English
English
 Français
Français
There are now more than 100 peer-reviewed science and medical journal articles that demonstrate the benefits of BrainHQ brain fitness technology. Currently, 60+ articles address benefits to people undergoing normal healthy aging, while 40+ discuss the impact on people with health conditions (eg, brain injury, mental illness, neurodegenerative disease). This report summarizes clinical evidence on improvements in healthy aging. Citations appear in brackets, below, and tie to the 60+ journal articles listed at the end.
Taken as a whole, the 60+ journal articles measuring the impact of Posit Science exercises on normal aging indicate that doing these exercises not only delivers measurable positive results, but also improves the overall trajectory of aging. In brief, the studies show that these exercises improve key standard measures of cognitive function (including, speed and accuracy of processing, attention, executive function and memory) [citations 1,2,3,4,5,6,28,48,49,50,51,56,60] as well as various standard measures of quality of life (including functional independence, feelings of control, depressive symptoms and health related quality of life). [7,8,9,10,11,12,13,14,15, 51]
The impact of these brain exercises on aging appears to be as broad and far-reaching as the impact of physical exercise, except the effects requires less time, diminish more slowly and impact the cognitive realm more deeply.
 All of the studies being reviewed are of exercises that are now commercially available solely from Posit Science, a mission-driven venture-backed company headquartered in San Francisco. Posit Science draws on a global network of university-based cognitive scientists to develop and test its computerized exercises. While other companies sell brain fitness products, very few of those have been submitted to any clinical testing and, to date, no others have been subjected to such extensive independent peer-reviewed trials. More information about Posit Science and its ongoing research and development can be found at www.dynamicbrain.brainhq.com.
All of the studies being reviewed are of exercises that are now commercially available solely from Posit Science, a mission-driven venture-backed company headquartered in San Francisco. Posit Science draws on a global network of university-based cognitive scientists to develop and test its computerized exercises. While other companies sell brain fitness products, very few of those have been submitted to any clinical testing and, to date, no others have been subjected to such extensive independent peer-reviewed trials. More information about Posit Science and its ongoing research and development can be found at www.dynamicbrain.brainhq.com.
All studies cited were (i) blinded, randomized controlled trials (the same type of study design used in drug trials), (ii) had results that were statistically significant and (iii) have been published in peer-reviewed journals. Except where otherwise explicitly noted, all studies involved just 10 hours of training with Posit Science exercises and were conducted by independent researchers, with no financial support from Posit Science.
Cognitive Gains
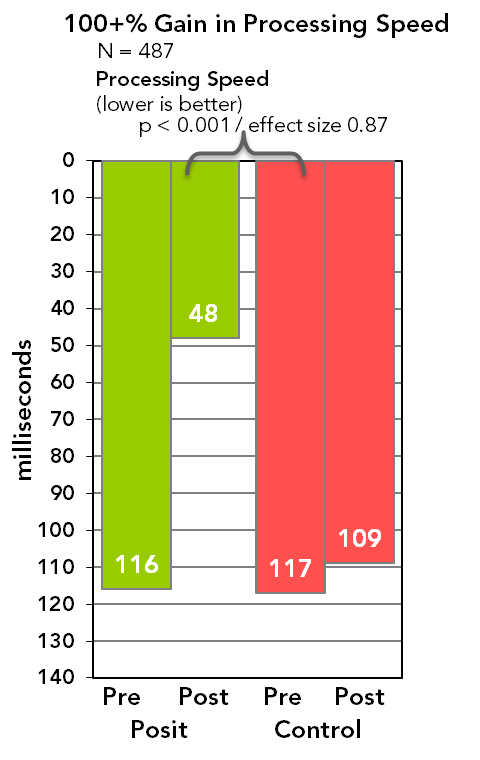
Speed of Processing. Numerous studies [1,2,4,5,6,48,49,50,51] now show that the exercises improve brain processing speed and accuracy. Two of the largest studies are the ACTIVE Study and the IMPACT Study. In the ACTIVE Study of 2,832 healthy adults aged 65 and older (conducted at six university and clinical sites), those doing the BrainHQ speed of processing training were shown to more than double the speed at which they could accurately process visual information, as compared both to the no contact control and to the two other experimental arms (which engaged in memory classes and reasoning classes for an equal amount of time) [9]. In a five-year follow-up, researchers found those who did extra “booster” sessions further countered age-related processing speed decline. [59] A study of 67 adults using a suite of BrainHQ visual exercises for 20 hours found similar gains to ACTIVE.[63] In the IMPACT Study of 487 healthy adults aged 65 and older (led by researchers at the Mayo Clinic and USC and with sponsorship by BrainHQ), participants who did auditory training exercises on their own at home for 40 hours, were shown, on average, to have more than doubled the speed at which they could process auditory information, as compared to little change in the active control arm (which did computer-based learning) [1]. The improvements were wide-spread, with some 93% showing speed of processing gains. In other studies, researchers have found that gains are unrelated to self-efficacy scores [62] or visual impairments. [61]
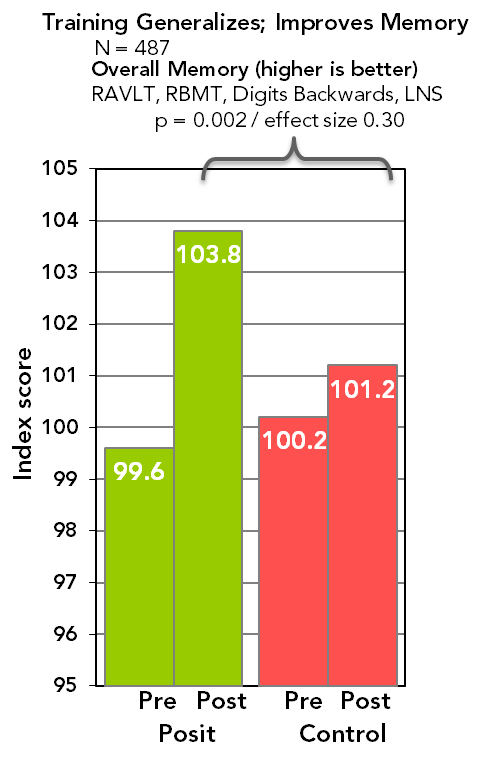 Memory and Attention. In the past, cognitive training exercises have been shown (at best) only to help people improve at the task trained and have been criticized because the training does not generalize. In the IMPACT Study, generalized improvements were shown for the first time (in any cognitive training program) in attention and memory (in both the primary and the secondary test batteries). These improvements, on average, were about 0.25 standard deviations, which is both clinically and statistically significant. In lay terms, 0.25 standard deviations is about the amount of decline that healthy adults over age 50 experience each decade on these standardized tests. This caused the researchers to observe that the participants saw gains of about 10 years, on average – making a 75 year old operate more like she did at 65 or an 85 year old more like he was at 75, etc.[1] Two earlier smaller studies (conducted by BrainHQ) with 72 and 161 participants produced similar results. [3, 28] An imaging study of 15 healthy adults aged 60 and older (conducted at UCSF with support from BrainHQ) used advanced EEG technology and showed increased activity in the areas of the brain associated with gains in working memory.[2] Another EEG study showed gains in attention.[56] In 2013, some of the researchers behind ACTIVE released study results for the IHAMS Study, which looked at 681 patients aged 50 and older, and which pitted users of a BrainHQ exercise against a control group doing crosswords.[50] They found 1.5 to 6.6 years of gain across a range of standard cognitive tests one year after participants had completed just 10 hours of brain exercises, and no gains for the crosswords group. They also found younger participants (50-64) did just as well as older participants (65+) despite less age-related impairment in the younger group. In addition, these researchers found people training on their own at home did just as well as those in a supervised setting. Another 58-person study, on selective visual attention, found users of a BrainHQ exercise significantly outperformed two active controls using the video games Tetris® and Medal of Honor®.[60]
Memory and Attention. In the past, cognitive training exercises have been shown (at best) only to help people improve at the task trained and have been criticized because the training does not generalize. In the IMPACT Study, generalized improvements were shown for the first time (in any cognitive training program) in attention and memory (in both the primary and the secondary test batteries). These improvements, on average, were about 0.25 standard deviations, which is both clinically and statistically significant. In lay terms, 0.25 standard deviations is about the amount of decline that healthy adults over age 50 experience each decade on these standardized tests. This caused the researchers to observe that the participants saw gains of about 10 years, on average – making a 75 year old operate more like she did at 65 or an 85 year old more like he was at 75, etc.[1] Two earlier smaller studies (conducted by BrainHQ) with 72 and 161 participants produced similar results. [3, 28] An imaging study of 15 healthy adults aged 60 and older (conducted at UCSF with support from BrainHQ) used advanced EEG technology and showed increased activity in the areas of the brain associated with gains in working memory.[2] Another EEG study showed gains in attention.[56] In 2013, some of the researchers behind ACTIVE released study results for the IHAMS Study, which looked at 681 patients aged 50 and older, and which pitted users of a BrainHQ exercise against a control group doing crosswords.[50] They found 1.5 to 6.6 years of gain across a range of standard cognitive tests one year after participants had completed just 10 hours of brain exercises, and no gains for the crosswords group. They also found younger participants (50-64) did just as well as older participants (65+) despite less age-related impairment in the younger group. In addition, these researchers found people training on their own at home did just as well as those in a supervised setting. Another 58-person study, on selective visual attention, found users of a BrainHQ exercise significantly outperformed two active controls using the video games Tetris® and Medal of Honor®.[60]
Executive Function. Researchers in the IHAMS Study found that participants involved in visual training improved in a number of standard measures of executive function – the ability to categorize, plan, reason and decide. [50] The IMPACT Study showed similar results for auditory training. [1]
Participants in the IMPACT Study were also assessed for improvements in everyday cognitive function. This involved having participants respond to a normed questionnaire about their abilities at everyday cognitive tasks (eg, “I remember names of people I meet,” “I have trouble following conversation in a noisy restaurant”). Those who did the exercises showed significant gains as compared with the control arm.[1] The results across all primary measures of the IMPACT Study (ie, processing speed, memory and attention, and everyday cognition) caused the researchers to observe that (i) people got better at what they trained at, (ii) those gains generalized to improvements in memory and attention and (iii) people said they noticed the changes in their daily lives. Researchers at Northwestern, in 2013, reported on significant improvements in key measures of hearing (speech in noise, auditory memory), as well as other cognitive abilities, among those who used auditory exercises from BrainHQ, and no significant gains in the active control, which engaged in computerized learning.[48, 57] A second study substantially replicated these results. [58] In a 2014 study, researchers found visual performance improved in both participants with normal and impaired vision after training with a BrainHQ exercise. [61] A look at pre-mature aging of the brain among people living with HIV, by researchers at the University of Alabama, found that speed and everyday function was significantly improved.[49]
 Functional Gains
Functional Gains
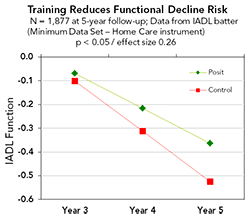
Functional Independence. ACTIVE Study researchers followed 2,832 participants for ten years to observe changes in functional independence (as measured by Instrumental Activities of Daily Living, or IADLs, such as ability to balance a checkbook or drive a car) after just 10 hours of training at the start of the study. Those who did the exercises had significantly less decline in functional independence than the no contact control over a five-year period, demonstrating a change in trajectory over the period.[9] A 10-year follow-up is the first to show long-term persistence of between group differences, despite benefits waning without further training. [51] Three other studies found that participants who did the exercises improved on a standard measure (timed IADLs), which predicts future performance on IADLs.[7, 8, 49, 64] These studies are also noteworthy because performance on measures of functional independence – IADLs – is also predictive of future performance at Activities of Daily Living or ADLs, a measure used for nursing home admission and long term care insurance claim eligibility.
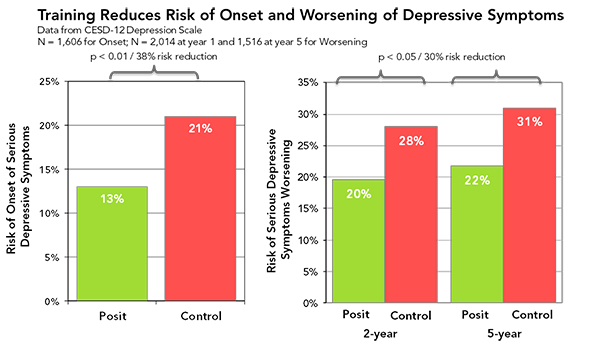
Mood and Control. A study of 1,534 participants showed, on average, that those who did the exercises felt greater control over their lives and more confidence in their everyday activities than those in the control group.[14] Those differences persisted over a five-year period even though training was just 10 hours at the beginning of the study. The ACTIVE Study (looking at 1,606 participants with no depression at baseline) found that those who did the exercises were 38% less likely a year later to experience onset of clinically significant depressive symptoms.[13] Similarly, looking at 1,516 subjects over a five-year period, they found those who did the exercises were 30% less likely to have a clinically significant worsening of depressive symptoms on the subsequent test date (at years 2 and 5).[12]
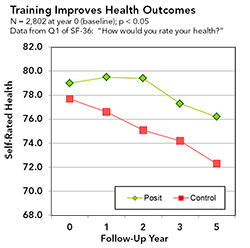
Health Outcomes. The ACTIVE Study also used a standard measure of Health Related Quality of Life or HRQoL (ie, the SF-36), which is used in most studies conducted by Medicare or the VA, to determine if the intervention noticeably helped the patient’s general health. Looking at 1,804 participants at the two-year and five-year follow-ups, they found 38% and 26%, respectively, reductions in risk of serious decline in HRQoL when compared to the other arms. [10,11] They also found that while the self-rated health (using the SF-1) of the participants in the other arms declined each year, the self-rated health of those who did the exercises followed a much better trajectory - actually improving for two years before beginning to decline - and with a significantly better endpoint at five years.[15] Using a model developed at DHS for predicting Medicare expenses based on SF-36 results, researchers found that those who did the exercises, on average, would have 3.3% lower annual Medicare expenses (about $300 per patient less, at today’s expense levels) than participants in the other arms. They also found that a between group difference persisted five years after the training, even as it waned without further training. [16]
Mobility Improvements
In addition to finding the gains in cognition and health outcomes cited above, researchers have also found BrainHQ technology is useful for measuring and improving mobility, which is a key element to healthy aging. [17,18,19,29,30,31,32,33,34,35,36,37,38,39,40, 41,42,43,44, 45,46, 47,52,53,55] The ACTIVE Study followed 908 participants for five years with access to their DMV driving records and found that those who did the exercises had 48% fewer “at fault” crashes than the other arms.[47] That’s with just 10 hours of training at the beginning of the five-year period. This confirmed earlier studies indicating that those with poor performance in the training tasks (about a third of older adults) had twice the crash risk.[29,30,33,36,39,40,43] In the SKILL Study, researchers sorted drivers into high and low risk and trained half the low risk drivers. Researchers were able to show that they could drive 9 of 10 high risk drivers to be low risk with just 10 hours of training [18]. They were also able to show that the trained drivers maintained their driving, as measured by distance, frequency and difficulty of driving conditions. This means they drove more and had fewer accidents. They were also 40% less likely to stop driving, and driving cessation has been shown to increase morbidity.[19] In addition, those who trained improved their reaction time by enough to gain 22 feet of stopping distance at 55mph. In an on-road driving safety study, those who did the brain exercises had 36% fewer dangerous maneuvers than the control who spent an equal amount of time in traditional drivers education.[17] Those who did poorly in the initial assessment were also found to be at greater risk of crashes at intersections and at higher risk for walking difficulties and falls [44,45,46] and more susceptible to driving cessation.[55] Two studies in the Chicago area showed improvements in balance and reductions in fall risk. Thirty hours of visual exercise training of older adults drove large and significant benefits in balance and reduction in fall risk, while a more impaired subset showed similar benefits in gait and reduction of mobility risk.[52] Twenty hours of training in a second study showed reduced fall risk and improved gait speed.[53]
How It Works
These results indicate that there is something special about the BrainHQ exercises. There are more than 100 issued patents with more than 1,000 patent claims underlying the technology in these exercises. Cognitive scientists from around the world have brought their best ideas to this work and look to make each part of every exercise as powerful as possible, so explaining how they work in a comprehensive manner is daunting.
Simply put, however, the exercises are based on a handful of powerful ideas. Unlike previous cognitive training, they do not try to fix a problem by practicing it – eg, they don’t improve memory by practicing memory. Instead, the exercises start with elemental cognitive function by first improving the speed and accuracy of your sensory perceptions. This becomes the foundation for improved attention. Improved attention is the building block of working memory, and working memory is the building block of pretty much everything else – immediate memory, delayed memory, episodic memory, executive function, reasoning, speech and language, visual-spatial skills, etc. No one has taken this complete bottom up approach to cognitive training before.
In addition, our scientists are experts in brain plasticity, the ability of the brain to re-wire and change. Each exercise draws on what experts have learned in recent years about driving change in the brain. Training needs to be focused on improving speed to meet varying real world conditions; it needs to intensively and progressively improve accuracy; it needs to be adapting continuously and minutely (eg by thousandths of a second) to each person’s performance and ability (based on algorithms that review all prior exercises results); it needs to be designed so the task gradually generalizes to real world experience; it needs to be engaging in a manner that naturally stimulates neurotransmitters (chemicals in the brain that enhance attention, learning and mood) and that brings you back to do the exercises again and again.
Who will it help?
Most studies to date have focused on people aged 60 or 65 and older, although recent studies have now replicated these results in people aged 50 and older. Researchers have sliced the data by age, gender, ethnicity, education level, socio-economic status and starting point and have not found any of those characteristics to be highly correlated to gain. What has correlated to gain is how far a user advances in the stimulus set underlying the exercises, which is good news, since that suggests it is the right stimuli. This means that, while individual results will vary, virtually everyone over 50 can experience gain from these exercises, and, on average, they do.
What’s Next?
Posit Science maintains an active research and development effort, with new exercises and new studies. Currently, there are more than 100 published journal articles on the benefits of these exercises, with dozens of other studies underway or completed and on their way to publication. Our research efforts also are applying this technology to a number of cognitive disorders (eg, psychotic illness, brain injuries and dementia).
Citations
1. Smith, G. E., Housen, P. et al. (2009). A cognitive training program based on principles of brain plasticity: results from the improvement in memory with plasticity-based adaptive cognitive training (IMPACT) study. J Am Geriatr Soc, 57(4), 594-603.
2. Berry, A.S., Zanto, T.P. et al. (2010). The Influence of Perceptual Training on Working Memory in Older Adults. PLoS One, 5:7, 11537.
3. Mahncke, H. W., Connor, B. B.et al. (2006). Memory enhancement in healthy older adults using a brain plasticity-based training program: a randomized, controlled study. Proc Natl Acad Sci U S A, 103(33), 12523-12528.
4. Ball, K.K., Beard, B.L.et al. (1998). Age and visual search: expanding the useful field of view. J Opt Soc Am A, 5(12), 2210-2219. [PMID:3230491]
5. Ball, K., Berch, D. B. et al. (2002). Effects of cognitive training interventions with older adults: a randomized controlled trial. JAMA, 288(18), 2271-2281.
6. Vance, D., Dawson, J. et al. (2007). The Accelerate Study: The Longitudinal Effect of Speed of Processing Training on Cognitive Performance of Older Adults. Rehabil Psych; 52(1):89-96.
7. Edwards, J.D., Wadley, V.G. et al. (2002). Transfer of a speed of processing intervention to near and far cognitive functions. Gerontology, 48(5), 329-340.
8. Edwards, J.D., Wadley, V.G. et al. (2005). The impact of speed of processing training on cognitive and everyday performance. Aging Ment Health, 9(3), 262-71.
9. Willis, S.L., Tennstedt, S.L. et al. (2006). Long-term effects of cognitive training on everyday functional outcomes in older adults. JAMA, 296(23), 2805-14.
10. Wolinsky, F. D., Unverzagt, F. W. et al. (2006). The effects of the ACTIVE cognitive training trial on clinically relevant declines in health-related quality of life. J Gerontol B Psychol Sci Soc Sci, 61(5), S281-7.
11. Wolinsky, F.D., Unverzagt, F. W. et al. (2006). The ACTIVE cognitive training trial and health-related quality of life: protection that lasts for 5 years. J Gerontol A Biol Sci Med Sci, 61(12), 1324-29.
12. Wolinsky, F.D., Vander Weg, M.W. et al. (2009). The effect of speed-of-processing training on depressive symptoms in ACTIVE. J Gerontol A Biol Sci Med Sci, 64A(4), 468-72.
13. Wolinsky, F.D., Mahncke, H.W. et al. (2009). The ACTIVE cognitive training interventions and the onset of and recovery from suspected clinical depression. J Gerontol B Psychol Sci Soc Sci, 64B(5), 577-85.
14. Wolinsky, F.D., Vander Weg M.W.et al. (2009). Does Cognitive Training Improve Internal Locus of Control Among Older Adults? J. Gerontol B Psychol Sci Soc Sci, 2010 Sep;65(5):591-8. doi: 10.1093/geronb/gbp117.
15. Wolinsky, F.D., Mahncke, H.W. et al. (2009). Speed of processing training protects self-rated health in older adults: enduring effects observed in the multi-site ACTIVE randomized controlled trial. Int Psychogeriatr. 2010 May;22(3): 470-8. doi: 10.1017/S1041610209991281.
16. Wolinsky, F.D., Mahncke, H.W. et al. (2009). The ACTIVE cognitive training trial and predicted medical expenditures. BMC Health Serv Res. Jun 29;9:109.
17. Roenker, D. L., Cissell, G. M.et al. (2003). Speed-of-processing and driving simulator training result in improved driving performance. Hum Factors, 45(2), 218-33.
18. Edwards, J.D., Myers, C. et al. (2009). The longitudinal impact of cognitive speed of processing training on driving mobility. Gerontologist, 49(4), 485-94.
19. Edwards, J.D., Delahunt P.B. et al. (2009). Cognitive speed of processing training delays driving cessation. J Gerontol A Biol Sci Med Sci. Dec;64(12):1262-7.
20. Scalf, P.E., Colcombe, S.J. et al. (2007). The neural correlates of an expanded functional field of view. J Gerontol B Psychol Sci Soc Sci, 62 Spec No 1, 32-44.
21. Ball, K.K., Edwards, J.D. et al. (2007). The impact of speed of processing training on cognitive and everyday functions. J Gerontol B Psychol Sci Soc Sci, 62 Spec No 1, 19-31.
22. Vance, D.E. (2009). The Emerging Role of Cognitive Remediation Therapy. Activities Adaptation & Aging, 33(1), 17-30.
23. Vance, D.E. (2009). Speed of processing in older adults: a cognitive overview for nursing. J Neurosci Nurs. Dec;41(6):290-7.
24. Vance, D.E., Wright M.A. (2009). Positive and negative neuroplasticity: implications for age-related cognitive declines. J Gerontol Nurs. Jun;35(6):11-17.
25. Vance, D.E., McNees P., Meneses, K. (2009). Technology, cognitive remediation, and nursing: directions for successful cognitive aging. J Gerontol Nurs. Feb;35(2):50-6.
26. Vance, D.E., Webb, N.M. et al. (2009). Mental stimulation, neural plasticity, and aging: directions for nursing research and practice. J Neurosci Nurs. Aug;40(4): 241-9.
27. Zelinski, E.M. (2009). Far transfer in cognitive training of older adults. Restor Neurol Neurosci. 27(5):455-71.
28. Mahncke, H.W., Bronstone, A., & Merzenich, M.M. (2006). Brain plasticity and functional losses in the aged: scientific bases for a novel intervention. Prog Brain Res, 157, 81-109.
29. Owsley, C., Ball, K. et al. (1991). Visual/cognitive correlates of vehicle accidents in older drivers. Psychol Aging, 6(3): 403-15.
30. Ball, K., Owsley, C. et al. (1993). Visual attention problems as a predictor of vehicle crashes in older drivers. Invest Ophthalmol Vis Sci, 34(11): 3110-3123.
31. Goode, K.T., Ball, K.K. et al. (1998). Useful field of view and other neurocognitive indicators of crash risk in older adults. Journal of Clinical Psychology in Medical Settings; 5(4):425- 40.
32. McGwin, G., Jr., Owsley, C. & Ball, K. (1998). Identifying crash involvement among older drivers: Agreement between self-report and state-records. Accid Anal and Prev; 30(6): 781-91.
33. Owsley, C., Ball, K. et al. (1998). Visual Processing Impairment and Risk of Motor Vehicle Crash Among Older Adults. JAMA: 279:1083-1088.
34. Owsley, C., McGwin G., Jr. & Ball, K. (1998). Vision impairment, eye disease, and injurious motor vehicle crashes in the elderly. Opthalmic Epidemiol 5(2): 101-13.
35. Myers, R.S., Ball, K et al. (2000). Relation of useful field of view and other screening tests to on-road driving performance. Percept Mot Skills, 91(1): 279-90.
36. Sims, R.V., McGwin, G Jr. et al. (2000). An exploratory study of incident vehicle crashes among older drivers. J Gerontol Med Sci; 55A:M22-M27. [PMID: N/A]
37. Sims, R.V., Owsley, C. et al. (1998). A preliminary assessment of the medical and functional factors associated with vehicle crashes by older adults. J Am Geriatr Soc, 46(5): 556–61.
38. Staplin, L., Gish, K.W., & Wagner, E.K. (2003). MaryPODS revisited: updated crash analysis and implications for screening program implementation. J Safety Res, 34(4), 389-97.
39. Clay, O.J., Wadley, V.G. et al. (2005). Cumulative meta-analysis of the relationship between useful field of view and driving performance in older adults: current and future implications. Optom Vis Sci, 82(8): 724-31.
40. Ball, K.K., Roenker, D.L.et al. (2006). Can high-risk older drivers be identified through performance-based measures in a Department of Motor Vehicles setting? J Am Geriatr Soc, 54(1): 77-84.
41. Pietras, T.A., Shi, Q. et al. (2006). Traffic-Entry behavior and crash risk for older drivers with impairment of selective attention. Percept Mot Skills, 102(3): 632-44.
42. Haymes, S.A., Leblanc, R. P. et al. (2007). Risk of falls and motor vehicle collisions in glaucoma. Invest Ophthalmol Vis Sci, 48(3): 1149-55.
43. Rubin, G.S., Ng, E. S. et al. (2007). A Prospective, population-based study on the role of visual impairment in motor vehicle crashes among older drivers: The SEE study. Invest Ophthalmol Vis Sci, 48(4): 1483-1491. [PMID: 17389475]
44. Broman, A.T., West, S.K. et al. (2004). Divided visual attention as a predictor of bumping while walking: the salisbury eye evaluation. Invest Ophthalmol Vis Sci. 45(9): 2955-60.
45. Owsley, C. & McGwin G. (2004). Association between visual attention and mobility in older adults. J Am Geriatr Soc. 52(11): 1901-6.
46. Vance, D.E., Ball, K.K. et al. (2006). Predictors of falling in older Maryland drivers: A structural-equation model. J Aging and Phy Act. 14(3): 254-69.
47. Ball, K., Edwards, J. et al. (2010), Cognitive Training Decreases Motor Vehicle Collision Involvement of Older Drivers. J Am Geriatr Soc, 58: 2107–11
48. Anderson, S., White-Schwoch, T. et al. (2013) Reversal of age-related neural timing delays with training, Proc Natl Acad Sci, doi:10.1073/pnas.1213555110
49. Vance, D.E., Fazeli, P.L. et al. (2012) Speed of processing training with middle-age and older adults with HIV. J Assoc Nurses AIDS Care, 23(6):500-10
50. Wolinksky, F.D., Vander Weg, M.W. et al. (2013) A Randomized Controlled Trial of Cognitive Training Using a Visual Speed of Processing Intervention in Middle Aged and Older Adults. PLOS ONE8(5): e61624. doi:10.1371/journal.pone.0061624
51. Rebok, G.W., Ball, K. et al. (2014) Ten-Year Effects of the Advanced Cognitive Training for Independent and Vital Elderly Cognitive Training Trial on Cognition and Everyday Functioning in Older Adults. J Am Geriatr Soc, 62(1): 16-24.
52. Smith-Ray, R.L., Hughes, S.L. et al. (2014) Impact of Cognitive Training on Balance and gait in Older Adults, J Gerontol Psychol Sci Soc Sci, doi:10.1093 /geronb/gbt097.
53. Smith-Ray, R.L., Makowski-Woidan, B.S. et al. (2014) A Randomized Trial to Measure the Impact of a Community-Based Cognitive Training Intervention on Balance and Gait in Cognitively Intact Black Older Adults, Health Educ Behav October 2014 vol. 41 no. 1 suppl 62S-69S
54. Zelinski, E.M., Peters, K.D. et al. (2014). Evaluating the relationship between change in performance on training tasks and on untrained outcomes, Front Hum Neurosci 8:617-51.
55. Ackerman AL, Vance DE et al (2014). What Factors Influence the Relationship Between Feedback on Cognitive Performance and Subsequent Driving Self-Regulation? J Appl Gerontol Apr 21. doi: 10.1177/0733464814529473
56. O’Brien JL, Edwards JD et al (2013) Cognitive training and selective attention in the aging brain: an electrophysiological study. Clin Neurophysiol. 2013 Nov;124(11): 2198-208
57. Anderson S, White-Schwoch T, et al (2014). Partial maintenance of auditory-based cognitive training benefits in older adults. Neuropsychologia 62: 286-296
58. Anderson S, White-Schwoch T et al (2013). Training changes processing of speech cues in older adults with hearing loss. Front Syst Neurosci 7:97
59. Ball KK, Ross LA, et al (2013). Speed of Processing Training in the ACTIVE Study: How Much is Needed and Who Benefits? Journal of Aging and Health 25(8_supp):65S-84S.
60. Belchior P, Marsiske M et al (2013). Video game training to improve selective visual attention in older adults. Comput Human Behav 29(4):1318-1324
61. Elliott AF, O’Connor ML et al (2014). Cognitive speed of processing training in older adults with visual impairments. Ophthalmic and Physiological 34(5).
62. Sharpe C, Holup AA et al (2014). Does Self-efficacy Affect Responsiveness to Cognitive Speed of Processing Training? J Aging Health 26(5):786-806
63. Edwards JD, Valdes EG et al (2013). The Efficacy of Insight Cognitive Training to Improve Useful Field of View Performance: A Brief Report. J Gerontol B Psychol Sci Soc Sci. DOI: 10.1093/geronb/gbt113
64. Edwards JD, Ruva CL et al (2013). An examination of mediators of the transfer of cognition speed of processing training to everyday functional performance. Psychology and Aging 28(2):314-321.